

Decoding Lower Extremity Wounds: The "Big Three" Ulcers Explained

Wounds on the legs and feet can be alarming, especially when they refuse to heal over weeks or months. For many patients, the immediate reaction is to simply clean the area, apply a generic antibiotic ointment, and wrap it tightly in a bandage.
However, in the world of advanced wound care, treating every leg wound the same way is a recipe for disaster.
The vast majority of chronic lower extremity wounds fall into one of three categories: Venous, Arterial, or Diabetic (Neuropathic). Because they are caused by completely different failures in the body's vascular or nervous systems, the treatment that heals one type can actually cause severe tissue damage to another.
Here is a breakdown of the "Big Three" and why an accurate clinical diagnosis must always come before the bandage.
1. Venous Stasis Ulcers: The Plumbing Backup
Venous ulcers are by far the most common type of lower extremity wound, accounting for roughly 70-80% of all cases.
They occur when the veins in your legs fail to pump oxygen-depleted blood back up to your heart. Because gravity is constantly pulling blood downward, faulty vein valves cause fluid to pool in the lower legs. This increased pressure causes fluid and proteins to leak into the surrounding tissue, eventually breaking down the skin from the inside out.
What they look like: Shallow, superficial, and irregularly shaped. The surrounding skin often looks dark red, brown, or stained (a condition called hemosiderin staining).
Moisture level: Highly exudative (they weep and drain heavily).
The Treatment Key: Compression. You have to fight gravity. Healing requires specialized, multi-layer compression wraps to physically squeeze the fluid out of the leg and back into circulation.
2. Arterial Ulcers: The Oxygen Drought
If venous ulcers are a plumbing backup, arterial ulcers are a severe drought.
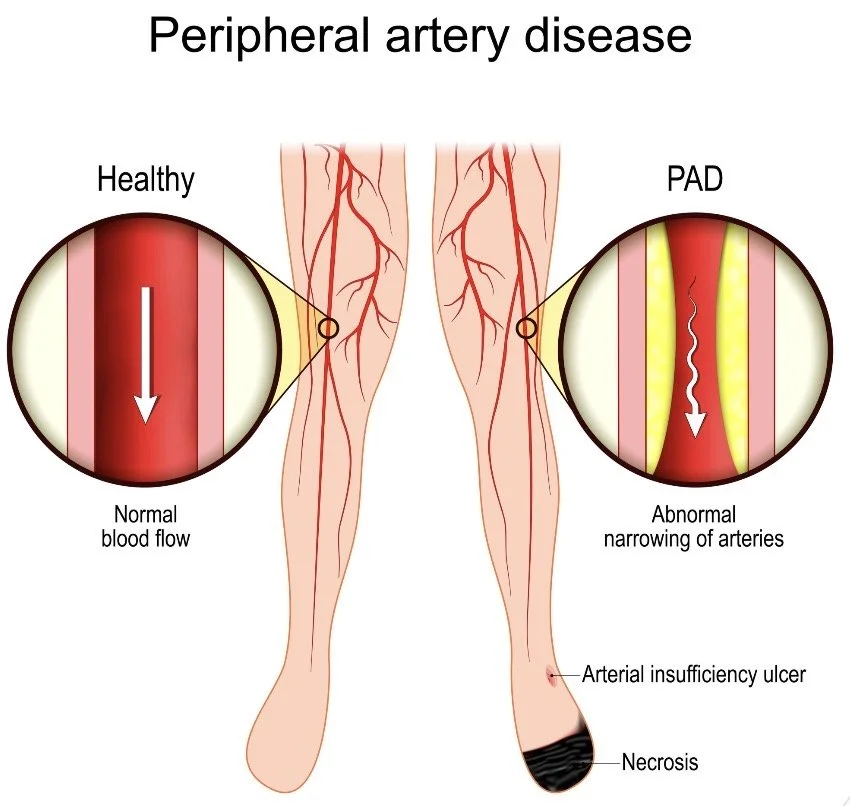
These wounds occur when oxygen-rich blood cannot reach the lower legs and feet, usually due to Peripheral Artery Disease (PAD) or severely clogged arteries. Without oxygen and nutrients, the tissue literally starves and dies.
What they look like: Deep, perfectly round ("punched out" appearance), with distinct, smooth edges. The wound bed is often pale, gray, or covered in black necrotic tissue.
Moisture level: Very dry.
The Treatment Key: Revascularization. The priority is restoring blood flow, often requiring a vascular surgeon.
The Diagnostic Danger: Never apply a compression wrap to an arterial ulcer. If the leg is already struggling to get blood, squeezing it with a tight compression wrap will cut off the remaining circulation entirely, leading to rapid tissue death or amputation.
3. Diabetic (Neuropathic) Foot Ulcers: The Silent Injury
Diabetic foot ulcers are caused by a combination of two diabetes-related complications: poor circulation and peripheral neuropathy (nerve damage).
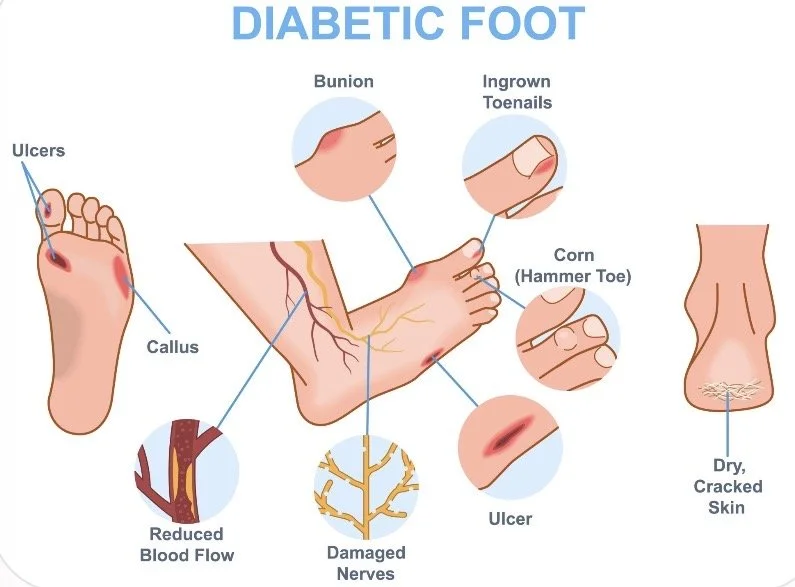
Because high blood sugar damages the nerves over time, a patient may completely lose feeling in their feet. They might step on a tack, wear shoes that are too tight, or develop a massive blister without feeling any pain whatsoever. The wound goes unnoticed, becomes infected, and rapidly deteriorates.
What they look like: Deep wounds usually surrounded by a thick, hardened callus.
Moisture level: Varies, but frequently complicated by underlying bone infections.
The Treatment Key: Offloading. You cannot heal a wound that you are constantly walking on. Treatment requires specialized boots, cast shoes, or total contact casting to completely remove pressure from the injured area.
Why Mobile Specialists Matter?
Correctly identifying the etiology (cause) of a wound requires advanced clinical training, specialized vascular assessments, and a deep understanding of tissue pathology.
At Vertex Wound Specialists, our mobile practitioners bring this diagnostic expertise directly to the patient's bedside. Before we ever apply a dressing, we assess the vascular status, the nerve function, and the tissue environment.
This ensures that every patient gets exactly the right intervention, whether that is advanced compression, targeted offloading, or an urgent vascular referral.
If you or a patient are struggling with a leg wound that simply isn't changing, stop guessing. Bring the specialist to the bedside and get the right diagnosis from day one.
